This blog will offer some expert recommendations to help guide the safety of hospital procedures at different platelet and coagulation profiles. Unfortunately, there are no strong evidence-based guidelines for hospital procedures dedicated to the study of patients with decompensated cirrhosis.
What is absolutely clear is that an elevated prothrombin time/INR does NOT predict the risk of bleeding with hospital procedures. An elevated PT/INR suggests that the levels of Vitamin K-dependent clotting factors (II, VII, IX and X) have decreased, but does not take into account the levels of protein C, protein S and antithrombin all of which also decrease in decompensated cirrhosis. Patients with decompensated cirrhosis have decreased levels of clotting and anticoagulation factors and increased von Willebrands Factor (vWF) and Factor VIII. This leads to a rebalanced hemostasis in decompensated cirrhosis so patients have as much a risk of bleeding as clotting. Cirrhotic patients are often mislabelled as being “auto-anticoagulated” implying an increased bleed risk because of an elevated INR. In actuality, 1% of patients with decompensated cirrhosis develop a deep venous thrombosis and/or a pulmonary embolus.1
The most recent Society of Interventional Radiology guidelines for Image-guided procedures has suggested the following recommendations summarized in Table 4 below2:
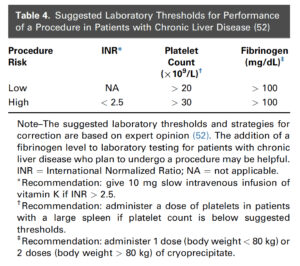
Reproduced from J Vasc Interv Radiol 2019; 30:1168–1184
Low-risk bedside procedures as defined by the Society of Interventional Radiology includes tube thoracostomy and the following ultrasound-guided procedures: central venous catheter placement, arterial line placement (<6 F), non-tunneled dialysis catheter placement, thoracentesis, paracentesis
High-risk bedside procedures as defined by the Society of Interventional Radiology includes lumbar puncture and solid organ biopsies
The above-mentioned suggested lab thresholds for image-guided procedures in patients with cirrhosis are based on expert opinion and low level evidence. The lab thresholds for low-risk procedures are similar to those in non-cirrhotic patients except for the need to keep fibrinogen levels >100 mg/dL. The PLT count requires a count >20K and any level of INR elevation if the INR is elevated solely from cirrhosis. We do know that these low-risk procedures can be performed on full anticoagulation or on dual antiplatelet therapy if necessary.2
For lumbar puncture, most guidelines recommend a PLT count at least 50K and an INR≤ 1.4-1.5 to safely perform a lumbar puncture. It is interesting that the SIR suggests safe performance if the INR<2.5 (from cirrhosis) and a PLT>30K. This is the one procedure that I would recommend a more conservative approach with a PLT count at least 50K and an INR≤ 1.4-1.5.
Although the safe thresholds for PT/INR and platelet threshold prior to performing a bedside procedure is not firmly established, what is clear is that FFP infusions to decrease the INR does not consistently decrease the bleed risk for bedside procedures and can cause harm. FFP can increase portal pressures in patients with cirrhosis and increase the risk of variceal bleeding.
With regards to thrombocytopenia in cirrhosis, the decreased platelet count is in part offset by increased platelet adhesion to injured endothelium by increased endothelial vWF. This is one reason why bedside procedures can be performed safely at PLT levels <50K.
A more accurate way to determine the bleed risk for bedside procedures in decompensated cirrhosis is to perform thromboelastogram (TEG) if available. Conservative TEG guidelines are to use a r > 40 min as indication for FFP and a MA < 30 for platelet transfusion.

Sources: