TOP TEN AIRWAY MANAGEMENT PEARLS TO OPTIMIZE YOUR CHANCES OF SECURING AN AIRWAY
- Develop a difficult airway management plan
- Huddle with your nurse and respiratory therapist in advance to alert everybody what plan A/B/C/D are for the patient
- If plan A is unsuccessful, move rapidly to plan B and then to plan C. Do not continue to attempt a technique that is not working
- Plan A may be to attempt direct laryngoscopy then plan B may be to attempt video laryngoscopy and plan C may be to place an intermediate airway (laryngeal mask airway or King tube) and plan D is to perform a surgical airway
- For all potentially difficult airways, identify and mark the incision point for a cricothyroidotomy if this were to be necessary.
- Have all of the equipment potentially necessary in the room immediately available
- Use a Straight-to-Cuff Stylet Shaping for Direct Laryngoscopy (DL) Intubations
- The shape of the stylet can impact the view of the larynx during direct laryngoscopy intubations
- A straight-to-cuff stylet shape can improve the laryngoscopic view during intubation attempts compared with the arcuate or curved stylet shaping
- Consider intubating in a semi-upright or reverse Trendelenberg position
- aFor morbidly obese patients, intubating in a semi-upright position increases the intubation time before desaturation by 30 seconds compared with supine intubations
- For patients with a potentially full stomach, intubating in a semi-upright position decreases the chance of emesis obscuring the intubation field and the chance of aspiration
- Think about your choice of intubation blades
- During video laryngoscopy, a standard geometry Macintosh-like blade is optimal for most patients unless they have limited neck mobility, possible C-spine injury or an anticipated anterior larynx (short thyromental distance or small mandible). The standard geometry blade provides an easier advancement of the endotracheal tube through the cords in most emergent intubationsb. A hyperangulated blade is optimal for a very anterior larynx or if there is limited neck mobility and possible C-spine injury when C-spine immobilization is held during intubation.
- Use enough neuromuscular blocker
- It is much easier to intubate a patient if they are paralyzed versus attempting a non-paralyzed intubation with only sedation (e.g., midazolam alone or etomidate alone). You will have a much higher first pass success rate if you perform rapid sequence intubation using a neuromuscular blocker
- Many airway management experts prefer rocuronium to succinylcholine in most circumstances
- If you will be using rocuronium, the use of 1.2 mg/kg leads to better visualization vs the use of 0.6 mg/kgd. Wait a full 60 seconds after the administration of rocuronium before attempting intubation (I always administer rocuronium before the induction agent such as etomidate to give it more time to work)
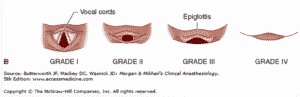
- Maneuvers to improve a Grade IV Cormack-Lehane (Laryngoscopic) View During Direct laryngoscopy
- Elevate the head on towels and extend the head to improve your sniffing position
- Advance the Macintosh blade to the tip of the vallecula before elevating the blade. The epiglottis should elevate more when the blade is elevated.
- Bimanual laryngoscopy with the right hand to grasp the tracheal cartilage and apply backward pressure and move the larynx side-to-side until the vocal cords/larynx come into view. Then have an assistant hold the tracheal cartilage in that position freeing up the right hand to grasp the endotracheal tube for intubation.
- If the epiglottis is not elevating despite advancing the blade to the tip of the vallecula, you can advance the whole blade under the epiglottis and elevate the epiglottis directly as you would with a Miller blade.
- Use Delayed Sequence Intubation for the Agitated Hypoxic Patient
- The agitated patient with hypoxic respiratory failure is challenging because they are often ripping off their mask or cannula during the preoxygenation phase.
- Use ketamine 1.5 mg/kg IVP as a dissociating dose to allow for preoxygenation
- Give glycopyrrolate 0.2 mg IVP as an antisialogogue to minimize secretions caused by ketaminec. After 3 minutes of preoxygenation, can give rocuronium and intubate the patient (ketamine acts as your induction agent)
- Have Push Dose Pressors Available for All Patients with Marginal Blood Pressures or Who Have a Physiologically Difficult Airway
- A physiologically difficult airway are conditions that carry the risk of hypotension or peri-intubation cardiac arrest: SBP<110; Severe hypoxic respiratory failure; Severe metabolic acidosis; and Right ventricular failure or moderate-severe pulmonary hypertension
- Push dose pressors can include epinephrine 1 mg diluted in 10 mL NS in a 10 mL syringe or phenylephrine 1 mg diluted in 10 mL NS
- My personal preference is to use phenylephrine and push 1 mL (100 mcg) q30-60 seconds for peri-intubation hypotension
- Would also prepare a norepinephrine drip and have it hanging so you can initiate it as well if peri-intubation hypotension occurs
- Order the ventilation analgesia and sedation drips at the time you order your intubating meds
- For patients who are hemodynamically stable, the most common analgesic will be a fentanyl drip
- For patients who are hypotensive, a ketamine drip can often improve the hypotension and provides analgesia
- For sedation, patients who are hemodynamically stable can usually tolerate propofol
- For patients who have severe delirium or are in the midst of substance abuse withdrawal (DTs or meth/cocaine withdrawal), dexmedetomidine can be used for sedation in addition to fentanyl
- Always have a bougie (Eschmann stylet) at the bedside for every intubation
- The bougie has saved me countless times when I have a Grade III-IV laryngoscopic view but can see the posterior corniculate tubercles or if I have a difficult time passing the endotracheal tube through the vocal cords
- Remember to keep the laryngoscope blade in the mouth to push the tongue anterior as you advance the endotracheal tube over the bougie
- If you have an NGT in place, do NOT put the bougie in the same hole as the NGT. Put the bougie anterior to the NGT.
Hope you find these airway pearls helpful. Please visit our whole repository of Hospital and Emergency Procedure blogs at https://hospitalprocedures.org/category/medical-procedures/ for evidence-based tips on all procedures performed in the ER, ICU and hospital wards! If interested in learning these procedures or refining your procedural technique, please consider registering for one of our Hospitalist and Emergency Procedures Courses at https://hospitalprocedures.org/course-registration/