Indications for a Thoracentesis
Indications for a Thoracentesis
– Work-up unexplained pleural effusion
– Rule out empyema
To relieve dyspnea and improve oxygenation
Contraindications for a Thoracentesis
– Uncooperative patient
– Overlying skin infection
– Ruptured diaphragm
– Small pleural effusion (≤ 1 cm on lat decubitus CXR)
– Loculated effusion
– Mechanical ventilation
– Coagulopathy (INR > 2.5 or PTT > 1.5 x upper limit NL)
– Thrombocytopenia (Platelets < 25K)
– Thienopyridine antiplatelet or DOAC use
– Severe uremia
Complications of a Thoracentesis
– Tube thoracostomy if symptomatic or > 15%
– 1/3 of all pneumothoraces require a chest tube
– Inexperienced operator (3.9% vs 8.5%)
– Therapeutic thoracentesis (OR 2.5)
– Mechanical ventilation (OR4, NS)
– >2 attempts (OR 2.5, NS)
– Manual aspiration
– Unlikely by limiting to removal of 1.5 L pleural fluid
– Avoid suction against excessive negative pressure
– Avoid entry sites below 8th ICS in midscapular line
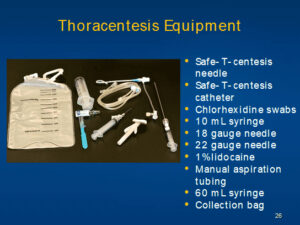
Equipment for a Thoracentesis
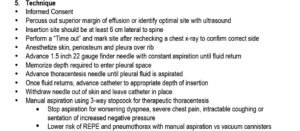
Proper positioning and technique for a Thoracentesis
Ultrasound-directed Thoracentesis
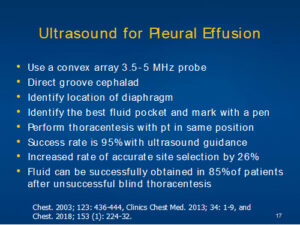
Ultrasound used to identify the optimal insertion location and then the patient is kept in the same position and the skin is then prepped with chlorhexidine and sterile drape applied
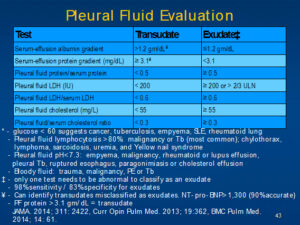
Pleural fluid analysis
Ultrasound used to identify the optimal insertion location and then the patient is kept in the same position and the skin is then prepped with chlorhexidine and sterile drape applied
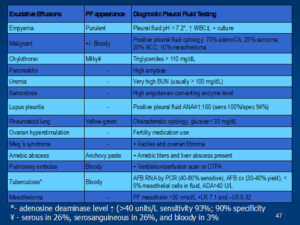
– Glucose < 60 suggests cancer, tuberculosis, empyema, SLE rheumatoid lung Pleural fluid lymphocytosis >80% malignancy or Tb (most common); chylothorax,lymphoma, sarcoidosis, uremia, and Yellow nail syndrome
– Pleural fluid pH<7.3: empyema, malignancy, rheumatoid or lupus effusion, pleural Tb, ruptured esophagus, paragonimiasis or cholesterol effusion
– Bloody fluid: trauma, malignancy, PE or Tb
– only one test needs to be abnormal to classify as an exudate
– 98% sensitivity / 83% specificity for exudates
– *Can identify transudates misclassified as exudates. NT- pro- ENP> 1,300 (90%accurate)
– PF protein > 3.1 gm/ dL = transudate
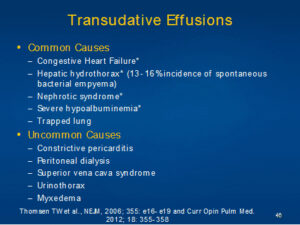
– Congestive Heart Failure*
– Hepatic hydrothorax* (13- 16 %incidence of spontaneous bacterial empyema)
– Nephrotic syndrome*
– Severe hypoalbuminemia*
– Trapped lung
– Constrictive pericarditis
– Peritoneal dialysis
– Superior vena cava syndrome
– Urinothorax
– Myxedema
Coding for a Thoracentesis
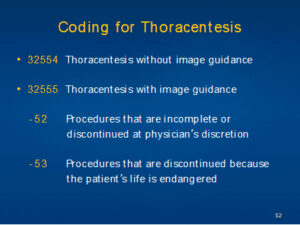
-52 Procedures that are incomplete or discontinued at physician’s discretion
-53 Procedures that are discontinued because the patient’s life is endangered