Indications for Ultrasound Guided Peripheral IV
Indications for Ultrasound Guided Peripheral IV
Ultrasound-Guided Peripheral IVs: An Alternative to Central Venous Catheters?Dr. Rick Rutherford, M.D., FAAFP
March 1, 2012
One of the most common indications for placing a central venous catheter is “no IV access”. I certainly have placed numerous central lines for this reason. Unfortunately, this practice is not without consequences. In addition to patient discomfort and mechanical complications, central line associated bloodstream infections (CLABSI) occur in U.S. hospitals approximately 250,000 times per year. By conservative estimates each CLABSI lengthens hospital stay by two weeks, increases cost by $30,000 and carries a mortality that ranges from 12 to 25%. CLABSIs can be reduced by adhering to proven practices during insertion and maintenance of central lines. However, there is also a direct correlation between CLABSI rates and a hospital’s device utilization ratio, defined as the number of central line days divided by the number of patient days in a hospital. Wouldn’t it be nice if we could just insert fewer central lines?
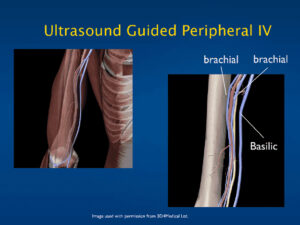
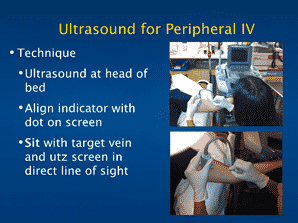
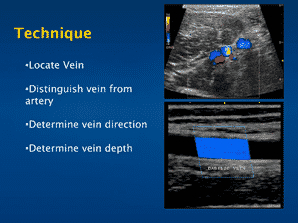
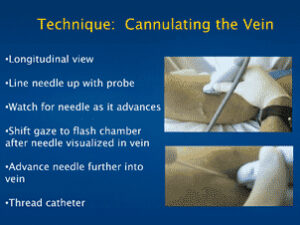
The use of ultrasound guidance for peripheral IV insertion has been described as early as the 1970s but has increased in the last eight years with the rise of point of care ultrasound.1 Most patients with difficult venous access lack visible, palpable veins near the surface of the skin. Edema, obesity, dehydration, IVDA and frequent venipuncture can all cause this problem. The ultrasound machine can be used to visualize veins deeper beneath the surface of the skin that are often larger, less mobile and have not been previously punctured. Ultrasound-guided peripheral IVs may be placed by physicians or nurses, can be learned quickly and have high success rates. In an ER setting, Bauman et al saw an 87% success rate among nurses placing ultrasound-guided peripheral IVs for difficult access patients.1 Gregg et al showed that in a mixed ICU over a 6 month period, 148 requests were received to place ultrasound-guided peripheral IVs after traditional IV access failed, and ultrasound-guided peripheral lines were placed successfully in 147 of those cases.2 While early studies showed low rates of “IV survival” when placed under ultrasound guidance, this problem has largely been eliminated by the use of longer IV catheters, with more of their length within the actual vein. Infection rates have been shown to be low and comparable to traditional IV insertion using standard aseptic technique. Finally patient satisfaction with this technique is high.3 Schoenfeld and colleagues surveyed patients who underwent ultrasound-guided peripheral IV insertion and found that the study population, 62% of whom had a central line placed in the past year, had an average satisfaction score of 9.2 out of 10.44
In my practice, I have found an important role for ultrasound-guided IV access. In the emergency department, the technique has allowed us to avoid placing central venous catheters in patients who otherwise wouldn’t need them. In the intensive care unit, ultrasound-guided lines are placed so that existing central lines may be removed. Both doctors and nurses have learned the technique and are inserting lines with high success rates. To learn more about ultrasound-guided peripheral IV insertion visit us at www.hospitalprocedures.org.
4. Schoenfeld et al. Ultrasound-guided peripheral venous access in the emergency department: A patient centered survey. Western Journal of Emerg Med. Nov, 2011:475-77.
Dargin et al. Ultrasonography-guided peripheral intravenous catheter survival in ED patients with difficult access. Am J Emerg Med. 2010 Jan;28(1):1-7