Eschmann stylets, or Bougies, can assist the clinician with endotracheal intubation in difficult airway scenarios. The stylet when properly placed can act to guide the endotracheal tube (ETT) into the trachea. However, there are different troubleshooting techniques that once must know about these intubating stylets to properly use them.
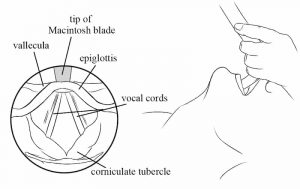
The ideal scenario for the Eschmann stylet, or bougie, is when the operator is performing direct laryngoscopy and can visualize the corniculate tubercles but not the vocal cords. Understanding that the corniculate tubercles lie just posterior to the vocal cords, the bougie can be advanced with the coude tip directed anteriorly just anterior to the corniculate tubercles. The bougie usually passes without resistance into the trachea in this scenario.
The Eschmann stylet can end up being placed in one of three locations: the esophagus, the ventricular folds or aryepiglottic folds, or the trachea. When the stylet is placed in the esophagus, it advances without resistance, has a smooth passage and never stops advancing. These are all bad signs and should trigger the thought in the operator that the tube is in the wrong location and should be withdrawn immediately. When the stylet is introduced and hits the ventricular fold or the aryepiglottic fold, it will stop early and abruptly right at the glottis. This is a clue that the stylet is lateral to the glottic opening and should be directed more medially and hopefully pass through the vocal cords. If the stylet is passed through the vocal cords into the trachea, the operator should feel “tracheal bumping” or a “washboard sign” as the stylet hits the anterior tracheal rings while passing down the trachea. In addition, the stylet will eventually stop when the coude tip hits a secondary bronchus causing the “hang up sign”. The “washboard sign” and the “hang up sign” are both reassuring indications that the stylet is in the proper location and can be used to direct the ETT into the proper location.
There are a few difficult scenarios that can occur with the Eschmann stylet that the clinician must be aware of. The first scenario is that the stylet can pass through the vocal cords but the tip can get stuck on a tracheal ring. If you see the stylet passing through the cords and gets stuck immediately after then you can rotate the stylet 90 degrees to the side or turn it 180 degrees so the coude tip is directed posteriorly and this should alleviate the problem. The stylet can also get hung up at the most anterior part of the vocal cords where they come together. The intervention in this case as well is to turn the stylet 180 degrees so the coude tip is directed posteriorly and this should solve the problem. Finally, the stylet can be properly placed in the trachea but the bevel of the ETT can become stuck on either the corniculate tubercles, the vocal cords, or on a tracheal ring. If this happens, remember the mantra “rings right” and turn the ETT 90 degrees to the right. This maneuver redirects the ETT bevel and should allow it to pass smoothly down into the trachea.