This blog summarizes a recent update reviewing current management recommendations for hepatic hydrothorax (HH). Hepatic hydrothorax is a complication of decompensated cirrhosis with portal hypertension. Sixty percent of patients accumulate both ascitic fluid and pleural fluid as a result of portal hypertension, but 40% of patients form pleural effusions in the absence of ascites. Sixty five percent of hepatic hydrothorax effusions are right pleural effusions, 20% of cases occur as bilateral effusions and only 15% of cases are left pleural effusions. The effusions are almost always transudative effusions by Light’s criteria but about 15% can be exudative especially in patients on chronic diuretics. The diagnosis requires excluding pulmonary and cardiac causes of a transudative effusion; however, a unilateral transudative right pleural effusion in a patient with decompensated cirrhosis is almost always HH.
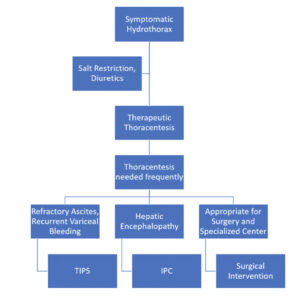
The pathophysiology of HH is thought to be from diaphragmatic fenestrations that allow seepage of fluid from the liver to travel up into the pleural space. The initial management of all HH is the same as the management of cirrhotic ascites: sodium restriction <2 gm/day and use of furosemide: spironolactone starting at 40 mg furosemide daily and 100 mg spironolactone daily and gradually increase these doses to a max of 160 mg furosemide and 400 mg spironolactone daily. For patients with refractory HH despite optimal medical management, you can perform serial therapeutic thoracentesis. In addition, all patients with decompensated cirrhosis and either ascites or hepatic hydrothorax should be referred to a liver transplant center for an orthotopic liver transplantation evaluation (OLT).
If patients are requiring frequent therapeutic thoracenteses, you have three options prior to OLT as shown in the figure below. A transjugular intrahepatic portosystemic shunt (TIPS) procedure is an option if the patient does NOT have CHF, pulmonary hypertension, hepatic encephalopathy or a MELD score>18. The success rate for a TIPS procedure has been reported between 58-73%. Surgical intervention with a VATS and pleurodesis +/- diaphragmatic defect repair with mesh is an option in appropriate surgical candidates. The success rate for surgery has been reported to be 45-73% and the 3-month mortality can be as high as 40%. Finally, an indwelling tunneled pleural catheter (IPC) can be placed but the infection rate ranges from 16-19% for these catheters.
The only cure for patients with decompensated cirrhosis with portal hypertension is OLT so all of these interventions are purely supportive in nature.
