Classification of Shock States:
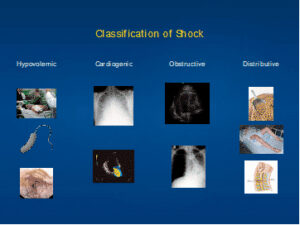
Classification of Shock States:
Goal Directed Ultrasound in Shock:
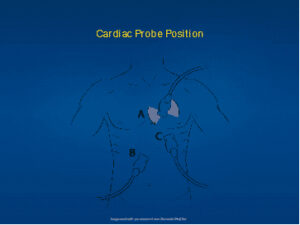
Cardiac Ultrasound:
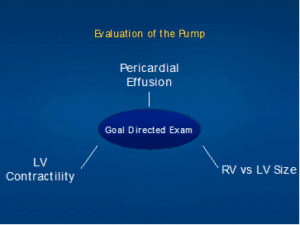
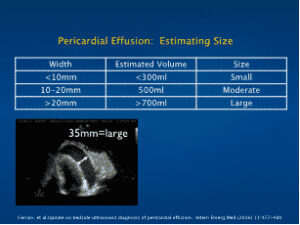
Pericardial Effusion:
Left Ventricular Dysfunction:

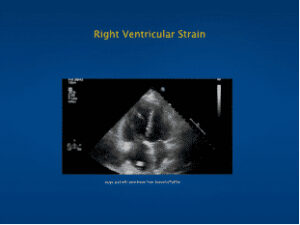
Right Ventricular Enlargement:
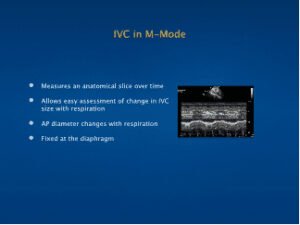
Inferior Vena Cava: Assessment of Volume Responsiveness
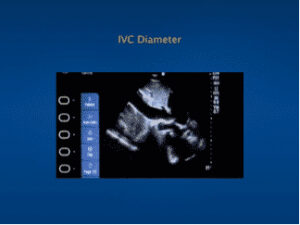
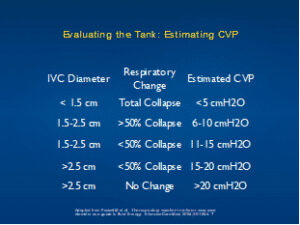
| IVC Diameter | Respiratory Change | Estimated CVP |
| < 1.5 cm | Total Collapse | <5 cmH20 |
| 1.5-2.5 cm | >50% Collapse | 6-10 cmH20 |
| 1.5-2.5 cm | <50% Collapse | 11-15 cmH20 |
| >2.5 cm | <50% Collapse | 15-20 cmH20 |
| >2.5 cm | No Change | >20 cmH20 |
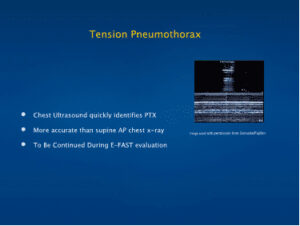
Obstructive Shock: Tension Pneumothorax
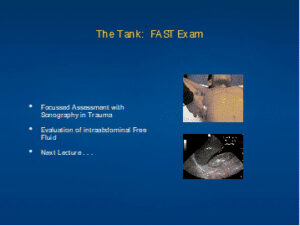
Distributive Shock: Focused Abdominal Sonography in Trauma
Aortic Pathology:
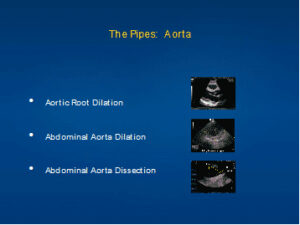
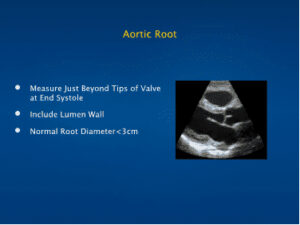
Aortic Root Measurement:
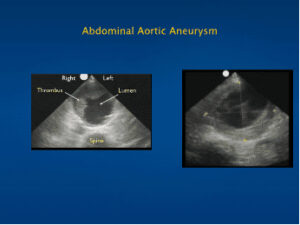
Aortic Aneurysm:
Aortic Dissection:
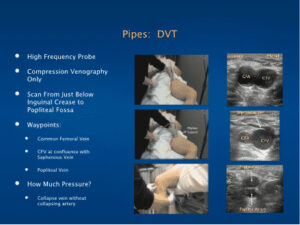
Deep Vein Thrombosis:
Putting it all together:
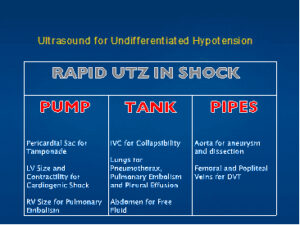
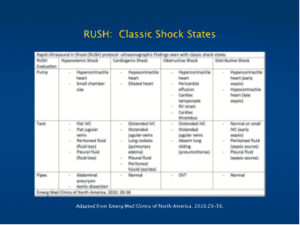
| PUMP | TANK | PIPES |
| Pericardial Sac for Tamponade |
IVC for Collapsibility | Aorta for aneurysm and dissection |
| LV Size and Contractibility for Cardiogenic Shock | Lungs for Pneumothorax, Pulmonary Embolism and Pleural Effusion | Femoral and Popliteal Veins for DVT |
| RV Size for Pulmonary Embolism | Abdomen for Free Fluid |
USPSTF on screening for abdominal aortic aneurysm
Joseph Esherick, M.D., FAAFP, FHM
July 15, 2014
The USPSTF continues to recommend screening primarily in 65- to 75-year-old men who have ever smoked.
U.S. Preventive Services Task Force (USPSTF)
Background
Prevalence of abdominal aortic aneurysms (AAAs; defined by an aortic diameter of ≥3.0 cm) in adults older than 50 is as high as 7% in men and 1% in women. In 2005, the USPSTF recommended one-time screening by ultrasonography in 65- to 75-year-old men who had ever smoked (defined as having ever smoked ≥100 cigarettes) and recommended against routine screening in women (NEJM JW Gen Med Feb 18 2005). The USPSTF now has updated its recommendations.
Key Points
—Risk factors: Older age; positive smoking history; having a first-degree relative with AAA; and having a history of vascular aneurysms, coronary artery disease, cerebrovascular disease, hypercholesterolemia, obesity, or hypertension.
—As in 2005, the Task Force continues to recommend:
* One-time screening for AAAs with ultrasound in 65- to 75-year-old men who have ever smoked (Grade: B [recommend]).
* Selective screening for AAAs in 65- to 75-year-old men who have never smoked, if additional risk factors are present (Grade: C [recommend for selected patients]).
* No screening for women who have never smoked (Grade D: [recommend against]).
—The Task Force finds insufficient data to determine the balance of benefits and harms of screening for AAAs in 65- to 75-year-old women who have ever smoked (Grade: I [no recommendation]).
—Screening test: Abdominal duplex ultrasonography has sensitivity and specificity of 97% and 99%, respectively, and is the standard approach for AAA screening.
—Treatment:
* Refer patients with large AAAs (≥5.5 cm) for open repair or endovascular intervention.
* For smaller AAAs (3.0–5.4 cm), manage patients conservatively (e.g., with repeat ultrasonography every 3–12 months).
—Screening in men is associated with an absolute risk reduction in AAA-related death of 1.4 per 1000 men screened.

Reference:
LeFevre ML et al. Screening for abdominal aortic aneurysm: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2014 Jun 24; [e-pub ahead of print]. (http://dx.doi.org/10.7326/M14-1204)