A number of additional factors must be considered with airway management in COVID-positive patients. Hospital Procedures Consultants (HPC) can provide simulation-based training to prepare providers for airway management in COVID-positive patients. The first essential consideration is to place the patient into a negative pressure room prior to performing an airborne-producing procedure. Second, you need to protect yourself with adequate personal protective equipment (PPE). The third consideration is to minimize people in direct contact with COVID-positive patients requiring endotracheal intubation. In addition, intubations should be performed by the most experienced operator available and the technique for endotracheal intubation should be altered for both “standard intubations” and for difficult airway management.
The decision of when to intubate is a difficult decision and will vary from institution to institution. Many institutions are still choosing to perform early endotracheal intubation as soon as the patient requires more than 6 L/minute supplemental oxygen. This strategy was first implemented in China in February, but has not been universally adopted. Other institutions are managing many very hypoxic COVID-positive patients successfully using either High-flow nasal cannula (HFNC) or non-invasive ventilation (NIV) often obviating the need for intubation.
We have identified two phenotypes of symptomatic COVID-positive patients: the “Happy Hypoxic” patient and the patient in cytokine storm. The “Happy Hypoxic” patient may be severely hypoxic but appears clinically well with no increased work of breathing and frequently denies dyspnea. Conversely, the patients in cytokine storm are usually febrile, have tachycardia, tachypnea, dypnea and increased work of breathing. Patients in cytokine storm will require endotracheal intubation, but “Happy Hypoxic” patients can usually be managed with high-flow nasal cannula unless they develop a hyperinflammatory syndrome.
When patients need to be intubated, the following principles should be followed:
- Critical to have a code discussion as early as possible with patients experiencing hypoxic respiratory failure.
- Given the significant potential for spread to healthcare providers, would have a low threshold to declare elderly patients with comorbid conditions “Do Not Resuscitate” if they were to die from COVID.
- Would also determine a surrogate decision-maker if the patient does not have the capacity to do so
- Minimize spread – Try to use an aerosol-reduction cover and a non-rebreather mask to transport a patient to a negative pressure room
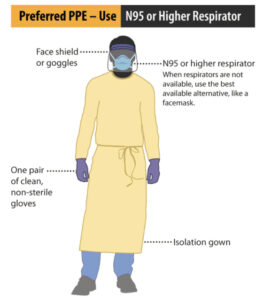
- Always protect yourself – Take your time to don adequate PPE before entering the room. This includes wearing an N95 respirator and a face shield or a PAPR (powered air-purifying respirator), full gown, head cover, and double gloves.
- Assure continuous cardiac and oximetry monitoring and frequent blood pressure checks
- Team huddle outside room to discuss airway management plans A, B and C and delineate clear team roles
- The most experienced air management expert should perform the intubation
- Minimize people in patient’s room – an intubation usually only requires the presence of an airway management expert and a respiratory therapist.
- An RN and an additional RT are usually in the ante-room in case the primary team requires additional equipment or assistance
- Assure adequate vascular access
- Bring all potentially needed equipment into room
- Recommend a Plexiglass barrier between intubator and patient
- Suction with Yankauer tip
- 10 mL syringe and endotracheal tube holder
- Direct laryngoscopy – laryngoscope and Mac 4 and Miller 3 blades
- Bougie
- Video laryngoscope with appropriate blade
- 0 and 7.5 endotracheal tubes with rigid stylet
- EtCO2 detector
- Bag valve mask connected in order to in-line HEPA viral filter then EtCO2 detector and then PEEP valve
- Rescue supraglottic tube (e.g., laryngeal mask airway, iGel or King tube)
- Bring all equipment and ultrasound needed for arterial line and central line placement post-intubation
- Orogastric tube and tape
- Assure that HEPA viral filter is attached to the expiratory limb of the ventilator
- If time allows, bring ventilator monitor/control panel to ante-room
- If time allows, bring IV pumps to ante-room connected to MRI IV tubing
- If time allows, get post-intubation sedation/analgesia medication drips primed
- Bring intubation medications into room
- Induction agent – etomidate or ketamine recommended
- Neuromuscular blocker – recommend rocuronium 1.2 mg/kg IVP
- Push dose pressor if post-intubation hypotension occurs
- Phenylephrine or epinephrine 100 mcg IV q30-60 seconds prn SBP<90
- Preoxygenation with head of bed at 45 degrees – recommend high-flow nasal cannula with overlying non-rebreather mask for 3-5 minutes if time allows
- Administer induction medication and neuromuscular blocker
- Allow for complete paralysis before attempt at intubation
- Avoid bag mask ventilation after neuromuscular blocker administered
- Recommend video laryngoscopy for initial intubation attempt with patient in semi-upright position
- Recommend placement of a supraglottic airway after two unsuccessful intubation attempts
- Front-of-neck-access (FONA) scalpel cricothyroidotomy only if absolutely necessary
- Connect ventilator airway tubing to endotracheal tube immediately after insertion
- Start ventilator sedation and analgesia infusions
- Place orogastric tube
- Arterial line placement +/- central line placement
- Chest x-ray for line/tube placement
References:
- Sullivan et al. In-hospital airway management of COVID-19 patients. Critical Care (2020) 24:292
- Wong P. et al. Aligning difficult airway guidelines with the anesthetic COVID‑19 guidelines to develop a COVID‑19 difficult airway strategy: a narrative review. Journal of Anesthesia. June 20, 2020 at https://doi.org/10.1007/s00540-020-02819-2